Katrine V. Løken
Joint work with Manudeep Bhuller and Laura Khoury
In our working paper ‘Prison, mental health and family spillover’, we find that the mental health of Norwegian inmates is much improved, up to five years after release from prison, compared to before the prison sentence.
Access to rehabilitation programmes while in prison is a key driver of the improved mental health. This is consistent with also observing positive effects on mental health for defendants receiving other punishments that also offer access to rehabilitation programmes, such as probation and community service. At the same time, we find no change in mental health for those getting a verdict of fine and no effect for a matched sample with similar characteristics that have never been charged. None of these latter groups got better access to rehabilitation programmes. For the partner of the offender receiving a prison sentence, we also see positive effects on mental health. This result is driven by partners separating upon the prison sentence, suggesting that the mental health of partners is improved by separating from a criminal partner.
In the US, the biggest mental health institutions, in terms of the number of individuals that have a mental health diagnosis, are prisons. More than half of US inmates have a mental health issue. In a survey conducted in Norwegian prisons in 2005, 76 per cent of inmates informed they had a mental health or drug related issue. In the US, the budgets are typically limited when it comes to treating mental health diagnoses. In Norway, to the contrary, there is much more emphasis on rehabilitation and treatment, as we will explain later in ‘Institutional details’. This is a likely explanation for why, in Norway, we find prison to have positive effects prison on mental health.
Method and data
Estimating the effects of prison is challenging. Firstly, it has been challenging to have data that register the crime and imprisonment and also follow the defendant (and partners) in the labour market, health outcomes and household structure over time. Secondly, prison entry is not random and can be correlated with unobservable characteristics of the family members.
This paper draws on multiple strengths of the Norwegian setting to overcome these challenges as we link several administrative data sources and construct a panel with complete records of criminal behaviour, prison time and health status for every Norwegian from 2006 to 2014. Using this panel data set, we can follow inmates for up to five years after the prison sentence, allowing us to assess their mental health outcomes over a prolonged period after release. We also look at outcomes for partners, children and parents. In addition, we use two different research designs to identify the causal effects of prison. First, we use an event study design that takes advantage of the variation in the criminal case decision date under the identifying assumption that the timing of the case decision is conditionally random. Second, we exploit a random judge design where we instrument prison sentencing decisions using variation in randomly assigned judges that differ systematically in their stringency.
Institutional details
The prison system in Norway emphasizes rehabilitation and follows the principle of normality set forth by the Norwegian Correctional Services. This principle dictates that “life inside will resemble life outside as much as possible” and that “offenders shall be placed in the lowest possible security regime.” This means that the main punishment is the restriction of liberty and that no other rights should be taken away from inmates serving time in Norwegian prisons. To promote and facilitate rehabilitation, prisons commonly offer education, mental health and training programmes. The mental health programmes are targeted at social or emotional skills such as anger management and interpersonal relationships, while other programmes aim to combat recidivism or drug addiction. All inmates are involved in some type of regular daily activity unless they have a serious mental or physical disability. If they are not enrolled in an educational or training programme, they must work within prison. After release, there is an emphasis on helping offenders reintegrate into society, with access to programmes set up to help ex-inmates find a job and access social services like housing support. On the health side, by law, prisoners have the same rights to healthcare services as the population at large.
Results
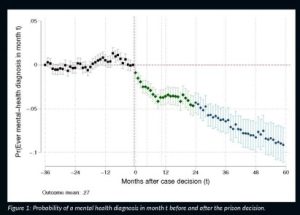
We offer three key findings. First, both the event study and the IV estimates reveal a large decrease in mental health-related visits for inmates that persist after their release. By contrast, the ordinary least squares (OLS) estimates show a positive association between imprisonment and subsequent mental health-related visits. For instance, the event study shows that imprisonment causes a 30 per cent decline in the probability of a mental health visit five years after the prison sentencing decision in court, while the OLS suggests a 14 per cent increase. Figure 1 illustrates the effect on defendants using the event study design.
Second, in interpreting the evidence, we find that incapacitation only explains a small share of the decline in mental health-related visits as the impacts persist and become stronger in the years after the inmate leaves prison. Furthermore, we observe a decline in both addiction and depression-related diagnoses, suggesting that the impacts extend beyond de-addiction. We also obtain evidence consistent with our estimates, reflecting an improvement in mental health and not merely a decrease in healthcare demand. Several pieces of evidence support this argument. First, inmates have a very high level of healthcare utilisation at the baseline and do not seem to distrust the healthcare system. The relatively humane prison conditions in Norway make it unlikely that prison negatively affects this trust. Moreover, we also observe a decline in emergency healthcare visits for mental health reasons, and we do not see any longer run upticks in mental health diagnoses even at five years after the prison sentence. The opposite could have been consistent with a short-term decline, resulting in longer-term increases in mental health problems. The absence of a decline in physical health-related visits also suggests that healthcare demand is not affected downward.
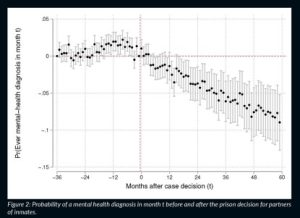
Finally, we find significant spillovers on spouses, for whom we also observe a large decrease in mental health-related visits. This is illustrated in Figure 2. At five years after the sentencing of the inmate, only about 40 per cent of inmates and their spouses are still together, and the spillovers to spouses are driven by those that split up. Children and parents also experience a decrease, albeit smaller, in mental health-related visits in the longer term. We also find a reduction in child protection-related incidents in these families. Taken together, spillovers to spouses and fewer child protection-related incidents in these families suggest that prison can have important positive spillovers on family health and wellbeing. The potential benefits of rehabilitation through improvements in mental health are, therefore, large and go beyond the direct effects on the inmates themselves.
What can we learn from this study? One general policy lesson is to look to Norway to understand more about the successful remedies to rehabilitate mental health issues in prison. However, there is an open question on whether it could be possible to find better ways of treating the mental health issue earlier such that the crime that led to the prison sentence in the first place could have been avoided. More research is needed to understand these tradeoffs.
References
Bhuller, M., Khoury, L. and Løken, K. V. (2021) ‘Prison, Mental Health and Family Spillovers’, NHH Dept. of Economics Discussion Paper, 19.
Project name
CIVICS
Project summary
Overlooking victims of crime and their relationships to criminals has led to an incomplete and distorted view of crime and its individual and social costs. While a better understanding of these social interactions is crucial for designing more effective anti-crime policy, existing research in criminology, sociology and economics has struggled to identify causal effects due to data limitations and difficult statistical identification issues. This project will push the research frontier by combining register datasets that have never been merged before and by using several state-of-the-art statistical methods to estimate causal effects related to criminal peer groups and their victims.
Project lead profile
Katrine V. Løken is Professor of Economics at the Norwegian School of Economics. Her main work centres on early investments in children and the effects of different social policies. She has also studied the causal effects of incarceration. This ERC grant gives her the means of pushing the research frontier in the economics of crime with unique access to datasets on victims.
Contact details
View the Criminality, Victimization and Social Interactions project webpage for details on the team and how to contact us.
Funding
This project has received funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme under grant agreement No. 757279.
Image legends
Figure 1: Probability of a mental health diagnosis in month t before and after the prison decision.
Notes: Each dot shows the probability of a mental health diagnosis between inmates entering prison in
month 0 and inmates entering prison in month 60 (control group that only enters prison after our sample
period ends). The lines are 90 per cent confidence intervals. We see little difference between the treated and
control group in the years before the prison sentence starts for the treated (black); the difference opens when
entering prison (green) and continues to increase after exiting prison (blue).
Figure 2: Probability of a mental health diagnosis in month t before and after the prison decision for partners
of inmates.
Each dot shows the probability of a mental health diagnosis between partners of inmates entering prison in
month 0 and partners of inmates entering prison in month 60 (control group that only enters prison after
our sample period ends). The lines are 90 per cent confidence intervals. We see little difference between the
treated and control group in the years before the prison sentence starts and a clear difference after.